Each year, there are more than one million drug possession arrests in the United States, according to the Drug Policy Alliance. Some public health professionals argue that the criminal justice method to address drug use is not effective in fixing the problem. Instead, they suggest an alternative solution that focuses less on punishment of the individual and more on their health—the decriminalization of drugs.
Drug DecriminalizationDrugs & Alcohol
Mar 28, 2026-10 MIN READ
PublicHealthDegrees.org is owned by 2U, LLC, parent company of edX. Our goal is to help learners make confident, informed decisions about their education and career. Some programs shown here are offered by universities that partner with 2U, for which 2U provides marketing and operational support and receives compensation. Other programs shown may be paid advertisements from third parties. Both types of programs are identified with the word AD or Advertisement. We aim to keep information current and accurate. Learn more about edX and our partners.
The Drug Policy Alliance notes that annual drug possession arrests have often topped one million in the U.S., though totals vary by year and reporting. Some public health professionals argue that the criminal justice method to address drug use is not effective in fixing the problem. Instead, they suggest an alternative solution that focuses less on punishment of the individual and more on their health—the decriminalization of drugs.
What is drug decriminalization?
Drug decriminalization is the elimination of criminal charges for drug possession and individual use, possession of drug paraphernalia and low-level drug sales.
What is the difference between drug decriminalization vs. legalization?
Decriminalization is the elimination of criminal penalties for an activity while legalization eliminates all penalties. In places where drugs are decriminalized, individuals may face civil penalties for use or possession of a drug (e.g., fines or required counseling) but will not receive criminal charges, which can lead to incarceration and a criminal record.
By taking criminal charges off the table, advocates for drug decriminalization hope to decrease the stigma around drug use and guide people who use drugs toward treatment and support services instead of incarceration. Healthy People 2030 identifies incarceration as a significant social determinant of health, noting that involvement in the criminal legal system is associated with long-term impacts on economic stability, social support, and both physical and mental health outcomes.
However, this sort of policy change requires a nuanced approach and a comprehensive support system that recognizes the needs of individuals who use drugs. As public health professionals and other leaders explore the possibilities of drug decriminalization, it is important to consider the potential benefits and drawbacks of this approach and to understand the communities that are most affected by drug use.
Why Decriminalize Drugs?
There are many ways in which the criminalization of drugs affects public health. People who use illicit substances, including those experiencing substance use disorder, are often handled by the criminal justice system but not the healthcare system, which perpetuates problematic drug use and can lead to poorer health outcomes, including death.
“Drug policies that prioritise health and human rights are more effective and more humane.”
Out of the nearly 2 million people incarcerated in the United States, about one in five are held for a drug offense, according to the Prison Policy Initiative. When viewed through the lens of social determinants of health, incarceration is closely tied to health outcomes: the Vera Institute of Justice notes that incarcerated people experience higher rates of chronic medical conditions than the general population, and that the health impacts of incarceration extend beyond custody into families and communities.
When looking at the connection between health disparities and the criminalization of drugs, it’s important to consider who is most affected by enforcement and sentencing policies. By and large, drug law enforcement continues to fall disproportionately on communities of color. For example:
The Drug Policy Alliance reports Black people are 28% of those arrested for drug offenses, while making up about 14% of the U.S. population.
According to the CSG Justice Center, experiencing incarceration can negatively affect a person’s health and make it harder to regain a stable footing after release, especially in areas like employment, housing security, and health and well-being, which are widely recognized as core elements of successful reentry. These impacts can also extend to families. The American Bar Association notes that parental incarceration is considered an Adverse Childhood Experience (ACE) and summarizes research linking it to destabilizing, multi-generational harms for children and caregivers.
Health impacts show up during incarceration as well: Healthy People 2030’s incarceration literature summary reports that incarcerated men and women are more likely than the general population to experience chronic conditions such as high blood pressure, asthma, cancer, and arthritis, as well as infectious diseases, including HIV. And stigma and fear of legal consequences can discourage people from seeking care, something the CDC states plainly: “Stigma makes it harder for people with substance use disorders to get help.”
How Does Drug Decriminalization Work?
Supporters of drug decriminalization advocate for the elimination of criminal penalties for drug use and possession for personal use, and in some policies, possession of drug paraphernalia, while generally keeping drug production and sales illegal, according to the United Nations Office on Drugs and Crime.
By prioritizing health over punishment, these advocates suggest that decriminalization policies can help:
Reduce justice-system involvement for low-level possession and potentially free up public resources for other health and safety priorities.
Destigmatize drug use so individuals with substance use disorder feel safer seeking help
Reduce incarceration rates and the corresponding health risks
According to the CDC, decriminalization can also remove barriers to harm reduction, a public health approach focused on reducing the negative consequences of drug use through services that are intended to be accessible and nonjudgmental.
What Is Harm Reduction?
The goal of harm reduction programs and practices is to minimize the negative health effects of drug use, as well as the social and legal impacts of existing drug laws.
What is harm reduction?
Harm reduction services aim to minimize negative health outcomes associated with drug use, including overdose, death and infectious disease.
How does harm reduction work?
Instead of focusing on abstinence, harm reduction provides care to people who use drugs so they can do so more safely. An example of harm reduction is providing clean syringes to people who use drugs to minimize the risk of contracting HIV or another transmittable disease.
What are the types of harm reduction?
Types of harm reduction include overdose prevention and safer drug consumption services. Harm reduction programs may also offer referrals to treatment for individuals who are interested in achieving abstinence.
While harm reduction can include referrals to services for those who want to reach sobriety, the ideology does not make access to care conditional based on abstinence. Instead, it addresses harms related to problematic substance use through evidence-based interventions.
Examples of harm reduction include:
Syringe programs that provide access to clean needles and the means to safely dispose of them to reduce the transmission of diseases such as HIV
Safer drug consumption services, which provide designated sites for people to use pre-obtained drugs under the supervision of trained personnel
Locations for obtaining test strips for drugs that may contain traces of other substances, such as fentanyl, a synthetic opioid that is more likely to cause an overdose
Training and free access to Naloxone, a medicine that can reverse an opioid overdose
Weighing the Pros and Cons of Drug Decriminalization
Opponents of drug decriminalization often argue that removing criminal penalties could normalize or encourage continued drug use, according to the UN Office on Drugs and Crime. Supporters counter that criminalization has not eliminated substance use and that public health–oriented approaches may reduce harm. In practice, the potential benefits and drawbacks of decriminalization depend heavily on how policies are designed and implemented, because decriminalization is typically discussed as a shift away from criminal penalties for personal use and possession and toward health-centered responses that still require strong prevention, treatment, and support systems to function well.
Policy and research reviews also emphasize that impacts are not uniform across settings and can vary by context, service capacity, and the way reforms are structured, according to PLOS. The potential benefits and drawbacks of drug decriminalization depend heavily on how policies are designed and implemented; the United Nations Office on Drugs and Crime emphasizes that decriminalization should be accompanied by effective prevention strategies and access to an evidence-based continuum of treatment and care to achieve intended public health outcomes. Decriminalization can also remove barriers to harm reduction, which CDC describes as a public health approach intended to reduce harms (including overdose and infectious disease) through care that is designed to be free of stigma and centered on the needs of people who use drugs.
Drug Criminalization in the United States
On a federal level, use and possession of illegal drugs is a criminal offense in the United States. The determination of how drug use is regulated is based on The Controlled Substances Act, which puts controlled substances into five categories.
Schedule I drugs are defined as having no accepted medical use and a high potential for abuse.
Examples include:
Heroin
Lysergic acid diethylamide (LSD)
Cannabis, which the DEA currently lists as a Schedule I substance, although DOJ/DEA has pursued rulemaking to move marijuana to Schedule III.
Schedule III drugs are defined as having a moderate to low potential for physical and psychological dependence.
Examples include:
Ketamine
Anabolic steroids
Products containing less than 90 milligrams of codeine per dosage (e.g., certain cough syrups)
Schedule II drugs are considered to have a high potential for abuse and the potential for psychological or physical dependence.
Examples include:
Cocaine
Methamphetamine
Fentanyl
Oxycodone
Schedule IV drugs are considered to have low potential for misuse and low risk for developing dependence.
Examples include:
Zolpidem
Alprazolam
Diazepam
Schedule V drugs have an even lower risk for abuse. Substances in this category also consist of preparations with limited amounts of certain types of narcotics.
Examples include:
Diphenoxylate (anti-diarrhea medicine)
Pregabalin (nerve pain medication)
Products containing less than 200 milligrams of codeine
However, state laws vary on the level of criminalization, including Schedule I and Schedule II drugs, with some states moving toward decriminalization and/or defelonization, according to the Drug Policy Alliance.
Portugal implemented a nationwide shift away from criminal penalties for drug use in 2001 under Law No. 30/2000, which removed criminal sanctions for the use and possession of illicit drugs for personal use and routed these cases through an administrative/public-health response rather than the criminal courts. (Portugal, Law No. 30/2000) In the years since, Portugal’s drug indicators have not moved in a single direction across every measure or time period, so it’s best to describe outcomes as mixed and dependent on broader health-system investments; for up-to-date comparative context on drug use patterns and health harms across Europe (including Portugal’s national reporting), see the EUDA’s European Drug Report 2025.
Case Study: Drug Decriminalization in Portugal
Summary:
Portugal became the first country to decriminalize the use and possession of all illicit drugs in small amounts in 2001.
With this policy change, the country shifted from a criminal justice approach to a public health approach. Instead of facing incarceration for a drug violation, individuals are instead sent to a local commission consisting of a healthcare provider, lawyer and social worker, who provide information and access to treatment and medical services.
In tandem with the decriminalization of drugs, Portugal put funding toward treatment and harm reduction services for people who use drugs. These resources include safe syringe services and other strategies that allow individuals to consume drugs more safely.
Outcomes:
The decriminalization of drugs in Portugal has led to some significant gains in health outcomes for individuals who use drugs.
Portugal expanded access to treatment as part of its health-centered response; EUDA tracks treatment uptake through its Statistical Bulletin 2025 treatment demand datasets and the European Drug Report 2025 annex tables.
It is less clear how decriminalization affected overall drug-use prevalence, because rates vary by substance, age group, and survey year; the EUDA’s Statistical Bulletin 2025 compiles Portugal’s official, standardized indicators on prevalence and patterns of drug use over time. However, evidence on how decriminalization affects overall drug use is mixed, and changes in prevalence can depend on the drug, the population surveyed, and the broader treatment and prevention context.
What can be learned:
Portugal’s experience underscores that decriminalization is not a standalone fix—its public health impact depends heavily on implementation. The United Nations Office on Drugs and Crime (UNODC) emphasizes that decriminalization should be paired with effective prevention strategies and access to an evidence-based continuum of treatment and care in order to achieve intended health outcomes.
Portugal’s approach also suggests that decriminalization is not designed to end drug use. Instead, it can shift policy toward reducing harms and improving access to services, especially when reforms are coupled with treatment options and harm reduction interventions that reduce overdose and infectious-disease risk.
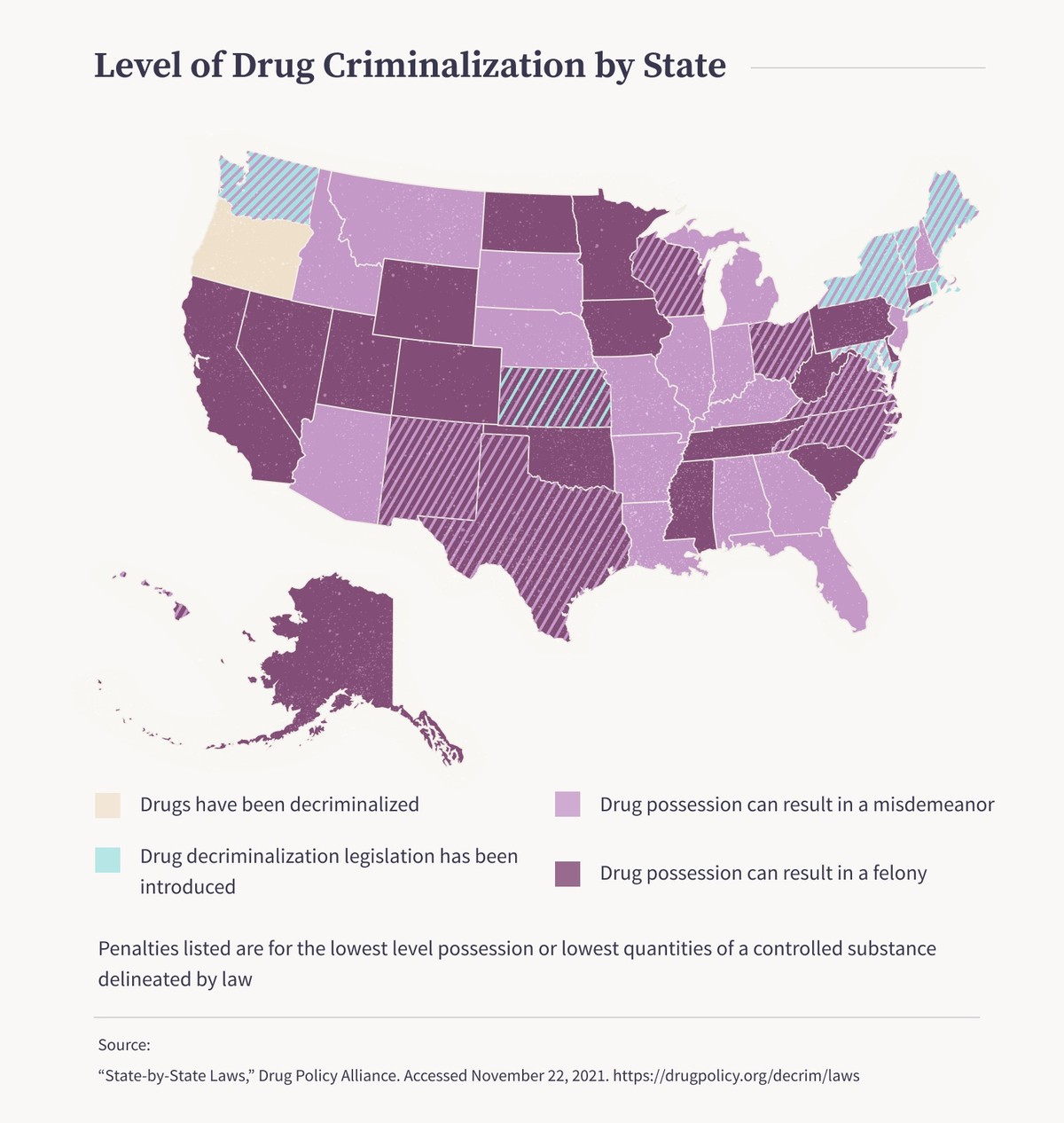
Level of Drug Criminalization by State
Because drug possession penalties change frequently across states, this guide uses a live policy tracker rather than a static state-by-state table. The Drug Policy Alliance maintains an interactive map that summarizes current state drug decriminalization and criminalization frameworks and is updated as laws change.
Important note: Oregon is a good example of why a static table can become outdated quickly: Oregon’s 2020 decriminalization policy was later reversed, and possession of small amounts of controlled substances was restored to misdemeanor status beginning September 1, 2024.
*Criminal charges can be a misdemeanor or a felony, depending on the circumstances.
Penalties listed are for the lowest level possession or the lowest quantities of a controlled substance delineated by law.